

Background
Multiple Myeloma (MM) is a plasma cell neoplasm causing a proliferation of monoclonal immunoglobulins that causes end organ damage in the form of hypercalcemia, renal insufficiency, anemia, and lytic bone lesions. Specifically, patients with MM are at risk for developing significant bone disease eventually leading to development of skeletal related events (SRE) (pathological fractures, spinal cord compression, and/or need for radiotherapy or surgery to bone). It is well established that the use of anti-resorptive agents (i.e. Bisphosphonates, Denosumab) lead to fewer bony lesions, less severe bone disease, and fewer SREs. However, while anti-resorptive therapy is recommended for all MM patients undergoing treatment, it is common for initiation of anti-resorptive therapy to be delayed due to the need for dental clearance, clinician preference, or relative contraindications to the medications. Current studies show that this therapy is overall underutilized, likely for similar reasons. However, the effect on SRE with regards to time to initiation of anti-resorptive agent has not been well studied. Herein, we conducted a retrospective analysis to determine if time to anti-resorptive agent has an effect on incidence of SREs.
Methods:
We performed a retrospective cohort study using our Electronic Health Record system to identify and analyze data of patients with newly diagnosed Multiple Myeloma from July 1st, 2016 until June 30th, 2019 to determine whether time to anti-resorptive therapy affects the incidence of SRE. Patients previously treated with bisphosphonates, and patients not treated with anti-resorptive therapy were excluded. The study's primary endpoint was probability of developing SRE based on time to anti-resorptive therapy. The relationship between incidence of SREs and time to anti-resorptive therapy, sex, age, ISS stage at diagnosis, Area Deprivation Index (ADI), and prior SRE present at diagnosis was analyzed by multivariable Cox proportional hazards model. The cutoff point of anti-resorptive therapy delay was based on the recursive partitioning of univariable Cox model.
Results:
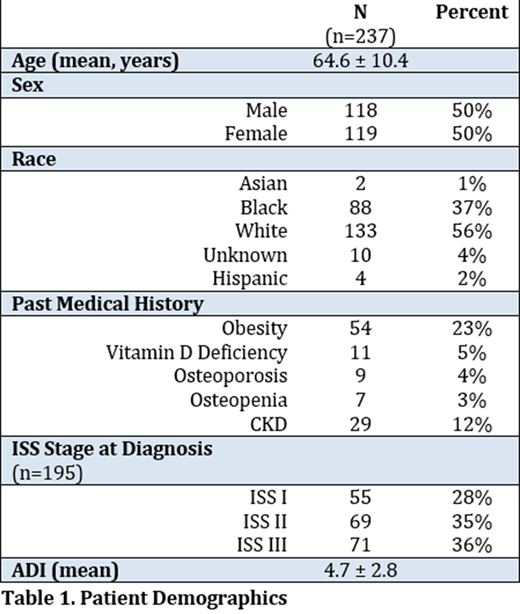
Three hundred and seventy-five patients with newly diagnosed multiple myeloma patients were identified. In total, 237 patients were included in the final analysis. Demographic information is detailed in the table provided. Of these, 208 patients (88%) used bisphosphonates and 29 (12%) used a RANK ligand inhibitor as their anti-resorptive agent. The median time to therapy was 55 days (IQR 135 days). One hundred twenty four (55%) patients had an SRE present at diagnosis. Forty-one (15.2%) patients developed a new SRE after initiation of anti-resorptive therapy. The model showed that patients who had a delay to anti-resorptive therapy of 31 days or greater had a higher risk of developing SRE after diagnosis (HR 2.49, 95% CI 0.95-6.55, p=0.064). In addition, when comparing ISS II to ISS I, patients with ISS II disease had a higher risk of developing SRE (HR 2.78, 95% CI 1.02-7.57, p=0.045).
Conclusions:
Patients with longer delays to anti-resorptive therapy had higher risk of developing SRE after diagnosis, however the difference was not statistically significant. One explanation for this may be that starting anti-resorptive therapy at any time point may be more important than time it takes to start therapy in the setting of effective anti-myeloma treatment. However, the rate of SRE in this study was lower than initially predicted based on previous studies, and therefore, our sample size may have been too small to detect a significant outcome related to time to initiation of anti-resorptive agents. Ongoing efforts to increase the sample size through multi-institutional initiatives are underway.
Binder:Janssen: Membership on an entity's Board of Directors or advisory committees; Sanofi: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal